Ebola, Africa’s Enduring Vulnerability, and the World’s Conditional Conscience
An Analytical Overview of the 2026 Bundibugyo Outbreak
By Silas Mwaudasheni Nande
Introduction: The Seventeenth Outbreak and Its Uncomfortable Truths
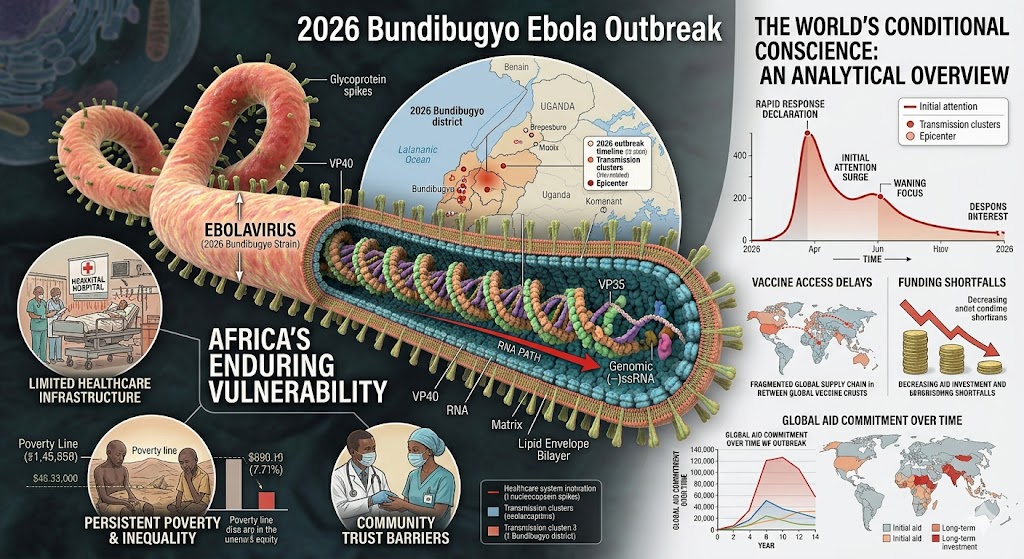
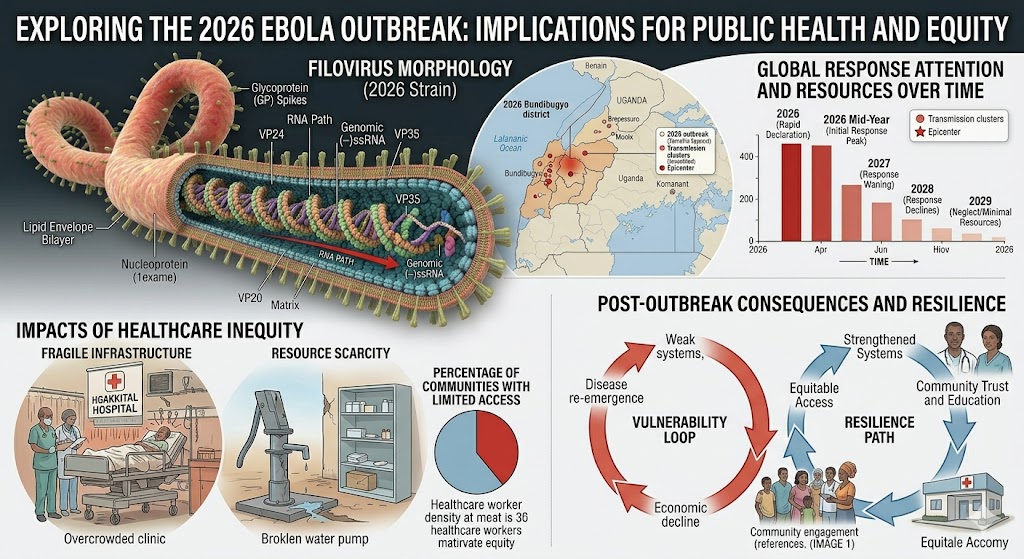
On 15 May 2026, the Democratic Republic of the Congo (DRC) confirmed its seventeenth Ebola outbreak, this time caused by the Bundibugyo virus, a genetically distinct strain with a case fatality rate of 30 to 50%, and, critically, for which no licensed vaccines or specific treatments currently exist. Within 48 hours, cases had crossed into Uganda, prompting the World Health Organization (WHO) to declare a Public Health Emergency of International Concern (PHEIC) on 17 May, citing unusual transmission patterns, high mortality, and the real risk of regional spread. By 20 May 2026, 342 suspected and confirmed cases and 89 deaths had been recorded across three health zones in Ituri Province, an area defined by dense population movement, cross-border trade networks, and severely limited health infrastructure.
This outbreak lays bare two fundamental and interrelated truths. First, Ebola is not a single solved problem but a family of evolving viral threats, and preparedness built around one strain can be rendered meaningless by another. Second, African nations remain structurally disadvantaged when confronting these threats, constrained by underfunded health systems, dependent on externally produced medical tools, and subject to the conditional attention of an international community that mobilises fully only when the virus appears to threaten Western populations. This analysis examines the nature of the Bundibugyo threat, the capacity deficits facing African nations, a concrete preparedness framework, and a critical assessment of whether Ebola genuinely ranks as a global priority.
Understanding the Threat: The Bundibugyo Strain and Why Africa Bears the Brunt
A Strain Without a Cure
Ebolaviruses comprise five distinct species: Zaire, Sudan, Bundibugyo, Tai Forest, and Reston. The Zaire strain is the most lethal and the most studied, with fatality rates reaching 90% in uncontrolled settings. Bundibugyo, first identified in Uganda in 2007 and again in the DRC in 2012, is less understood but presents unique challenges. Clinical data from the 2026 outbreak indicate more rapid disease progression in some patients, with higher rates of organ failure than previously observed.
The critical gap is this: all licensed vaccines, Ervebo and Zabdeno/Mvabea,and approved treatments, Inmazeb and Ebanga, were designed specifically against the Zaire strain. While laboratory studies suggest possible partial cross-protection, there is no clinical evidence that these products work against Bundibugyo. In practical terms, frontline responders in 2026 have no specific tools. They rely entirely on supportive care, infection control, and symptom management, measures that reduce mortality but cannot stop transmission. The 2026 outbreak thus validates what virologists have warned for decades: Ebola is a family of diseases, and a preparedness architecture built around one member of that family leaves the world dangerously exposed to all others.
Why Africa Carries the Burden
Since Ebola’s discovery in 1976, every major outbreak has originated in sub-Saharan Africa, with the DRC alone accounting for over 60% of all recorded cases and deaths. This is not coincidence. It reflects the convergence of three structural realities.
- Ecological exposure: African tropical forests are the natural reservoir for ebolaviruses, primarily carried by fruit bats. Deforestation, mining, and agricultural expansion, in Ituri Province, large-scale artisanal gold mining, drive humans into high-risk contact with wildlife, increasing spillover frequency.
- Health system fragility: The DRC has 0.8 doctors and 3.2 nurses per 10,000 people, less than one-tenth the ratio of high-income nations. Forty percent of its health facilities lack running water or electricity. Surveillance systems are weak; in 2026, three weeks elapsed from the first death to laboratory confirmation.
- Research and manufacturing dependency: No African country produces licensed Ebola vaccines or treatments. Every medical countermeasure must be imported, often arriving weeks after outbreaks have expanded beyond containment.
These factors combine to ensure that Africa faces the highest risk with the fewest resources to respond. When a new, untreatable strain emerges, the continent starts from a position of structural deficit.
Capacity Deficits: Why African Nations Cannot Yet Lead the Response
A defining characteristic of the 2026 outbreak is that most African countries remain unable to develop, produce, or deploy their own medical countermeasures. This is not a failure of intelligence or ambition; it is a failure of investment and infrastructure, accumulated over decades.
Research and Development
While the DRC’s Institut National de Recherche Biomédicale (INRB) successfully identified the Bundibugyo strain within 10days,a genuine achievement, it remains heavily dependent on external partners for reagents, sequencing equipment, and training. Across Africa, fewer than five countries can perform full genomic characterisation of filoviruses independently. No African-led clinical trial has yet produced a licensed Ebola product. R&D spending across the continent averages 0.4% of GDP, compared with 2.5% in high-income nations, and less than 5% of global health research funding reaches African institutions. Between 2014 and 2026, of 14 Ebola vaccines and therapies that reached advanced development, none were fully designed, tested, or manufactured in Africa.
Manufacturing and Supply Chains
No facility in Africa is currently licensed to produce viral-vectored vaccines, the platform underpinning all leading Ebola candidates. In every outbreak, vaccines, treatments, and personal protective equipment must be airlifted from Europe or North America. In 2026, initial supplies arrived 12 days after confirmation; by then, the virus had already spread to two additional health zones and crossed into Uganda. While WHO maintains an emergency stockpile, it is centrally managed and prioritised for global needs. African nations hold no collective reserve, meaning every outbreak starts from zero.
Health Systems and Operational Readiness
Africa carries 25% of the global disease burden but has only 3% of the world’s health workers. Four healthcare workers died in the first week of the 2026 outbreak due to inadequate infection prevention. Surveillance is fragmented; border protocols exist on paper but rarely in practice; and community trust, essential for contact tracing and safe burials, takes weeks to build in conflict-affected areas like eastern DRC. These are not merely technical gaps; they are the difference between a contained outbreak and a continental crisis.
A Framework for Preparedness: Five Strategic Pillars
Preparedness cannot be built during an emergency. The 2026 outbreak demands a structured, long-term response architecture. The following five pillars represent an evidence-based path forward, centred on the DRC and applicable across the continent.
Pillar 1: Build Endemic Research and Innovation Capacity
Scale up and sustainably fund institutions such as INRB, the Uganda Virus Research Institute, and the Kenya Medical Research Institute. Africa CDC should coordinate a network of 8 to 10 specialised research hubs with shared data and resources. Fully implement the African Medicines Regulatory Harmonisation initiative to reduce multi-country drug approval timelines from 24 months to 3 to 6 months. Support construction of at least two vaccine production facilities in Central and East Africa through technology transfer agreements. Upgrade INRB to serve as the regional reference laboratory for filoviruses, with the capacity to process 500-plus samples weekly.
Pillar 2: Strengthen Health Systems and Surveillance
Roll out digital surveillance across high-risk provinces in the DRC, linking community health workers, clinics, and laboratories in real time. Ensure every health facility has water, soap, PPE, and trained staff. Double the number of doctors, nurses, and laboratory technicians in high-risk regions, and create a regional reserve corps of 5,000 trained responders deployable within 48 hours. Establish 12 permanent diagnostic laboratories across eastern DRC, pre-stocked and satellite-connected to INRB. Community engagement is not peripheral to this effort; it is the strategy. No outbreak has been controlled without it.
 Pillar 3: Regional Cooperation and Cross-Border Preparedness
Pillar 3: Regional Cooperation and Cross-Border Preparedness
The Economic Community of Central African States (ECCAS) and the East African Community (EAC) should formalise binding protocols covering joint surveillance, shared stockpiles, rapid deployment, and coordinated communication. Two regional hubs, one in Central Africa, one in East Africa, should hold pre-positioned vaccines, diagnostics, and PPE, owned and managed by African institutions. Annual joint simulation exercises should involve health, transport, customs, and security agencies. The 2025 Sudan response showed that countries that rehearsed together responded 40% faster.
Pillar 4: Secure Access to Medical Tools Before Outbreaks
CEPI, WHO, and global manufacturers must be pressed to accelerate multivalent vaccines effective against all major Ebola species, including Bundibugyo and Sudan,the single most critical technical gap today. African governments should collectively negotiate pricing, supply guarantees, and technology transfer rights. Cold-chain infrastructure, currently insufficient for ultra-cold storage vaccines, must be expanded through solar-powered refrigeration and investment in heat-stable formulations.
Pillar 5: Sustainable Financing and Governance
African governments must honour the Abuja Declaration commitment of 15% of national budgets to health, with a dedicated percentage for preparedness. The DRC currently allocates just 7.2% to health overall. Africa CDC’s Africa Health Emergency Fund should be capitalised at US$500 million, enabling immediate fund release within 24 hours of an outbreak. International aid must include genuine capacity transfer, not only supplies or personnel.
The Global Agenda: Is Ebola Truly a Priority?
A fundamental question shapes this entire discussion: do Western nations treat Ebola as a genuine priority, or as a manageable threat to be contained at Africa’s borders? The evidence demands an honest, if uncomfortable, answer.
The Case for Engagement
Since the 2014–2016 West African epidemic that killed over 11,000 people, Western governments have invested substantially. The United States provided more than $6 billion for Ebola research, response, and preparedness between 2014 and 2026; the European Union contributed over €2.5 billion. The rVSV-ZEBOV vaccine, now the most widely deployed tool, was developed in Canada and advanced with American and European funding. Following 2014, Western nations drove reforms to global health security architecture, including the creation of CEPI and the Global Health Security Agenda. In every major outbreak since, Western experts, laboratories, and supplies have formed a substantial part of the international response. This engagement has been real and has saved lives.
The Case for Structural Neglect
Yet the factual record reveals an equally real pattern of conditional, biased, and insufficient prioritisation. Consider the following documented disparities:
- Funding volatility: Between 2021 and 2023, global Ebola preparedness funding fell by 75% as no major epidemic occurred. The US provided $1.2 billion for the 2014 outbreak response but averaged just $45 million annually for preparedness in the years that followed, a pattern that ensures countries are never fully ready when the next outbreak strikes.
- Research disparity: In 2025, global investment in influenza research exceeded $3.8 billion. Investment in all filoviruses combined was under $220 million. Between 2000 and 2025, only 4 of 1,400 newly approved medicines targeted Ebola or Marburg. The Bundibugyo and Sudan strains were identified in 2007 and 1977 respectively; vaccines for them entered serious development only in 2024.
- Political attention contingent on proximity: The 2014 epidemic became a top G7 agenda item only after a case appeared in the United States. The 2026 Bundibugyo outbreak received urgent UN Security Council attention only after modelling projected a 22% probability of spread to the Middle East and Europe. Outbreaks confined to African borders attract minimal high-level engagement.
- Technology hoarding: The licence for the rVSV-ZEBOV vaccine was held by a European company for over a decade. A full technology transfer to a South African manufacturer was completed only in 2024. When supplies are scarce, Western nations have historically secured national reserves, while affected African countries face shortages.
The 10/90 gap, 90% of health research funding targeting diseases affecting only 10% of the global population, remains fully operative for Ebola. Despite its devastating impact on Central Africa, the disease is classified as a “neglected tropical disease,” a categorisation that speaks volumes about whose suffering drives global priorities. African nations, despite bearing the disease burden, hold limited voting power in the WHO, CEPI, and World Bank governance structures where priorities are set.
Recommendations: A Shared Path Forward
For African Nations
- Assert ownership: Legally anchor INRB as the permanent regional leader in filovirus research. Through Africa CDC, adopt a binding Continental Health Security Strategy (2026–2035) establishing minimum standards for every member state.
- Invest in medical sovereignty: Allocate 2 to 3% of national health budgets to local research and manufacturing. Use the African Continental Free Trade Area (AfCFTA) to create a unified market that makes local production viable. Establish a US$1 billion African Biotech Fund to de-risk investment in vaccine and drug development.
- Formalise regional cooperation: ECCAS and EAC should create a permanent Central/East Africa Rapid Response Force with dedicated aircraft, mobile laboratories, and pre-deployed teams that are independent of international NGOs.
- Invest in community-led systems: In eastern DRC, formalise community health workers’ employment and integrate traditional leaders into the health governance structure. Trust is not a soft objective; it is the most powerful tool in outbreak control.
For Western Nations and Global Institutions
- Reverse the funding ratio: Commit 70% of health security funding to capacity building and 30% to emergency response, not the reverse. Multi-year grants of 5 to 10 years are essential; project funding cycles destroy institutional memory.
- End research bias: CEPI should launch a dedicated programme for neglected pathogens with regional risk, ensuring that Bundibugyo, Sudan, and Marburg receive equal priority to influenza or coronavirus. Treat vaccine knowledge as a global public good, not commercial property.
- Build partnerships, not dependencies: When deploying support, channel at least 60% of funds through local African institutions, not international contractors. Change the role of Western agencies from leading responses to equipping African responders.
- Reform global health governance: Support expansion of African nations’ voting weight and decision-making authority in WHO and CEPI, so that research and funding priorities reflect global health need, not geopolitical interest.
Conclusion: Preparedness Is Not Charity, It Is Shared Security
The emergence of the Bundibugyo strain in May 2026 is a stark reminder that Ebola has not been defeated; it has evolved. Each new outbreak tests a preparedness architecture that was built, imperfectly and incompletely, after the last crisis. The virus exploits every gap: in surveillance, in laboratory capacity, in manufacturing, in community trust, and in political will.
Africa’s vulnerability to Ebola is not inevitable. It is the accumulated result of underinvestment, structural inequity in global health governance, and a dependency model that has positioned African nations as recipients rather than architects of their own health security. The fact that no Ebola vaccine or treatment has ever been fully developed and manufactured on the continent is not a measure of African capability; it is a measure of how global priorities have been set, and by whom.
The international record is equally clear: Western engagement with Ebola has been significant, at times decisive, but it has been conditional. Resources and attention surge when the virus threatens non-African populations and contract when the crisis is contained to Central or East Africa. This is not a morally defensible model, and it is not a strategically sound one. In a world where a passenger can board a flight in Ituri and arrive in Paris, Frankfurt, or New York within 24 hours, health insecurity in one region is a potential emergency for all regions.
The 2026 outbreak is not simply another chapter in a long epidemiological history. It is a decision point. If African nations build the research capacity, manufacturing infrastructure, and regional solidarity that this moment demands, and if Western partners shift from reactive rescuers to genuine enablers, Ebola can be controlled not through luck or emergency mobilisation, but through sustained, equitable, and locally owned preparedness. The tools and knowledge exist. What remains to be tested is the political will to deploy them justly.
Similar Posts by The Mt Kenya Times:
- Diaspora Times Global June 13 – June 19, 2026
- Musk crosses the trillion-dollar threshold
- Rural stars head to Botswana for elite trials
- Africa’s Largest Bank Backs Dangote Refinery IPO
- The Silent Builders: Why Engineering Brilliance Needs a Social Megaphone